



Psychotic episodes don’t always mean chronic mental illness. Some people break from reality briefly before recovering completely.
Brief psychotic disorder catches families unprepared because symptoms hit fast and look frightening. Knowing what to watch for helps get proper care when episodes strike.
What Brief Psychotic Disorder Actually Means
Brief psychotic disorder happens when someone loses touch with reality for more than a day but under a month. That’s what defines it. Symptoms hit suddenly, sometimes in hours, then go away. Most people had no psychiatric problems before and return to normal after.
About one in 50,000 people get this each year, though real numbers are higher since many cases aren’t reported. Women are diagnosed slightly more often. It usually shows up between ages 20 and 35, but can happen at any age.
Doctors look at what triggered it. Sometimes major stress comes first – losing someone close, assault, disaster, or big life changes. Other times symptoms just appear without clear cause. Stress-related episodes tend to have better outcomes.
Symptoms and Duration of Brief Psychotic Disorder

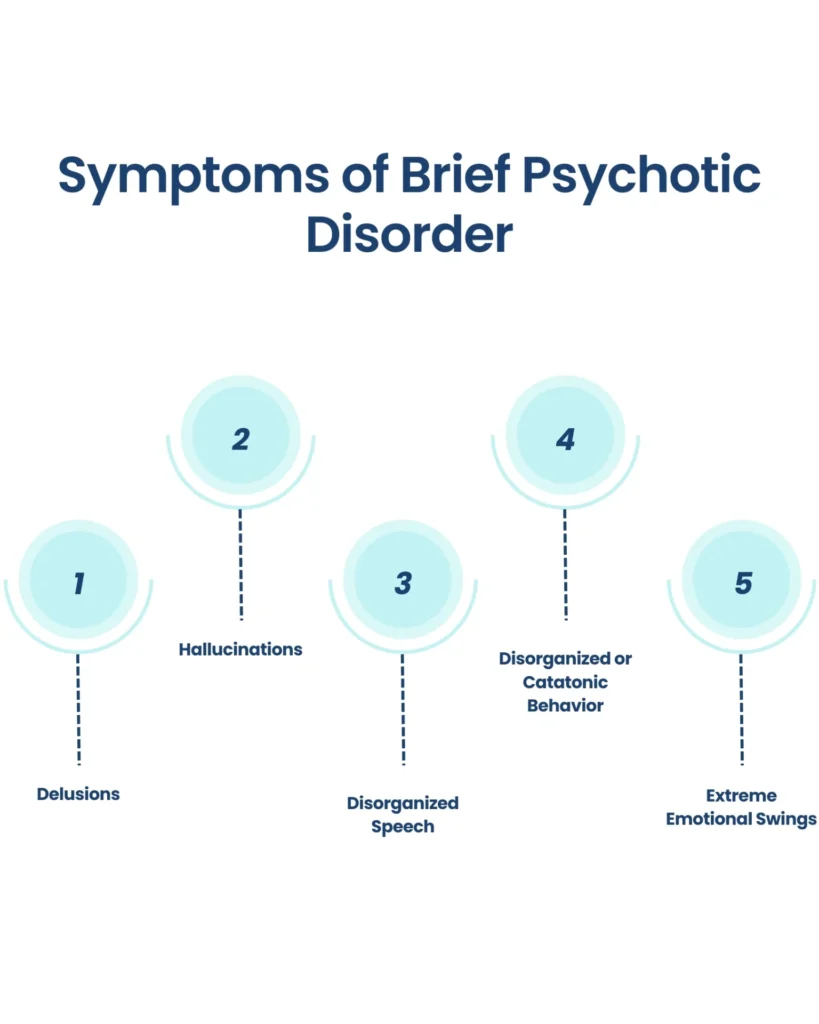
The most obvious ones include:
Hallucinations. Someone might hear voices, see things that aren’t there, or feel sensations on their skin even though nothing is touching their body.
Delusions. These are false beliefs that someone refuses to give up, even in the face of facts.
Other symptoms are:
- Disorganized thinking
- Speech or language that doesn’t make sense
- Unusual behavior
- Problems with memory
- Disorientation or confusion
- Changes in eating or sleeping habits, energy level, or weight
- Not being able to make decisions
Causes of Brief Psychotic Disorder

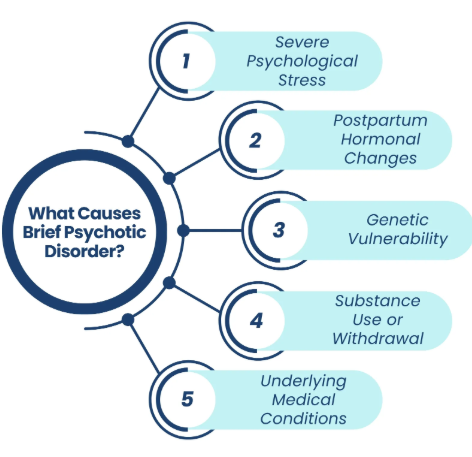
Experts don’t know what causes brief psychotic disorder. There may be a genetic link since the condition is more common in people who have a family history of psychotic or mood disorders, such as depression or bipolar disorder.
Another theory suggests that poor coping skills could trigger the disorder as a defense mechanism or an escape from a very frightening or stressful situation.
In most cases, the disorder is triggered by a major stress or traumatic event. Childbirth can be a trigger for some people.
Recognizing the Core Symptoms
Understanding Psychotic Experiences
Brief psychotic disorder symptoms look identical to other psychotic conditions. They just don’t last as long. Mental health professionals check for particular signs when someone might have this.
Hallucinations mean sensing things that aren’t real. Hearing voices when nobody’s talking is most common. Those voices might comment on what the person’s doing, bark orders, or talk amongst themselves. Some people see things no one else sees. Others feel bugs crawling on their skin or smell things that aren’t there. All of this feels absolutely real to them.
Delusions are beliefs that don’t match reality but won’t budge even with solid proof otherwise. Someone might insist they have special powers. Others become convinced people are plotting against them. Some see hidden messages in random everyday events meant specifically for them. These ideas completely take over how they think.
Disorganized speech happens when thinking gets so scrambled that talking stops making sense. The person jumps between topics without any thread connecting them, invents words, or speaks in ways nobody can parse.
Observable Behavioral Changes
Behavior shifts show up differently across people:
- Extreme restlessness where sitting still becomes impossible
- Bizarre actions that serve no purpose or don’t fit what’s happening
- Near-total immobility with almost no response to anything
- Holding weird body positions for long stretches
- Dangerous acts that put safety at risk
These symptoms wreck everything. Work can’t happen. Relationships crumble. Even eating or washing gets abandoned. The severity usually forces families to seek emergency psychiatric help.
If you’re dealing with this situation, getting hold of an optum psychiatrist or local emergency mental health services becomes the priority.
Duration of Brief Psychotic Disorder
How long symptoms persist is what makes this disorder “brief.” They need to last at least one full day to count. They also need to vanish completely within 30 days. Past one month, doctors start looking at other diagnoses like schizophreniform disorder.
Most people begin improving in the first week or two once treatment starts. The peak, when everything’s at its worst, typically runs several days to maybe two weeks. After that, symptoms gradually lift until the person’s back to baseline. That compressed timeline gives real hope versus conditions dragging on for months or years.
The duration of brief psychotic disorder also shapes treatment decisions. Shorter episodes, especially ones wrapping up in one to two weeks, usually point to better outcomes down the road. Episodes pushing close to 30 days sometimes hint at more chronic problems brewing, though that’s not guaranteed.
Getting Proper Treatment
Initial Crisis Management
Brief psychotic disorder treatment begins with making sure the person’s safe. Most need psychiatric hospitalization when symptoms are acute. During active psychosis, people can’t tell what’s real from what’s not. That’s dangerous – they might follow voices commanding self-harm, lash out based on paranoid beliefs, or forget to eat and drink.
Psychiatric wards provide locked environments with staff watching round the clock. Patients get monitored for how symptoms change, how medications work, and any safety issues. Hospitals strip away outside stress while stopping people from acting on dangerous urges.
Antipsychotic medications handle most of the treatment. These drugs block dopamine receptors in the brain, which lowers hallucinations, delusions, and disorganized thinking.
Psychiatrists typically start with newer medications like risperidone, olanzapine, quetiapine, or aripiprazole. These produce fewer movement side effects than older drugs, but often cause weight gain and metabolic problems.
Most patients see some improvement three to seven days after starting medication. Full recovery usually needs two to four weeks of steady treatment. Some bounce back remarkably fast – symptoms clearing in days. Others take the whole month even with proper medication dosing.
Duration of Medication Treatment
How long to keep taking antipsychotics after symptoms clear varies by person. Some psychiatrists push for three to six months post-recovery. That’s meant to prevent quick relapse while brain chemistry settles back down.
Other doctors lean toward shorter runs, especially when obvious stress triggered things and the patient’s clearly stable again. They might stop antipsychotics within weeks or months after symptoms vanish. That cuts exposure to medication downsides and recognizes most people never have another episode.
Making that call requires weighing multiple angles – did clear stressors exist, what’s the family psychiatric background, how fast did treatment work, what does the patient want, how bad are the side effects.
Therapy and Support
Therapy matters once acute symptoms calm enough for actual engagement. Individual therapy helps people process what just happened to them. Many feel bewildered about the whole thing, unsettled by memories of being psychotic, and scared it’ll happen again. Therapy gives space to sort through all that.
Cognitive behavioral therapy can tackle any leftover symptoms while teaching better stress management. Learning to spot early warnings of building stress or subtle symptom shifts allows faster action if trouble resurfaces. Building healthy ways to cope with pressure reduces chances of future episodes.
Family therapy or education helps relatives who are often scared and confused themselves. Understanding what brief psychotic disorder actually is, how it typically plays out, and what warning signs look like helps families support properly. It also stops them from either blowing off what happened or panicking over every tiny mood shift.
The Question of Recurrence
Can brief psychotic disorder come back? That question haunts patients and families post-recovery. Research offers some reassurance – studies peg it at roughly 50 to 80 percent having just one episode ever. Most people stay well permanently after their first episode and recovery.
For those getting hit with repeat episodes, patterns emerge. Recurrence usually happens when new severe stress appears, especially stress resembling what triggered round one. Someone whose first episode followed trauma might stay rock-solid for years until another trauma hits. That pattern suggests building solid stress management and processing hard experiences can cut recurrence risk.
Multiple factors shape whether symptoms might return:
- Episodes with clear major stress triggers typically fare better long-term than ones popping up without obvious cause
- Family history of psychotic or mood disorders ups genetic vulnerability for future episodes
- Fast, complete response to initial treatment generally forecasts better ongoing stability
- Continued exposure to heavy stress or unprocessed trauma can boost odds of additional episodes
- Substance use, especially stimulants or cannabis, might trigger recurrence in vulnerable people
Staying hooked into mental health services post-recovery helps outcomes. Regular follow-ups, even when feeling fine, let psychiatrists catch subtle early warnings. Jumping on things at the first whiff of returning symptoms can sometimes head off full relapse.
Recovery and Moving Forward
Most people return fully to pre-episode functioning after brief psychotic disorder clears. They go back to work or school without lingering problems. Relationships typically bounce back once families grasp what happened. Daily life resumes normally. That complete recovery separates this from chronic psychotic illnesses needing constant management.
Still, the psychological wallop of experiencing psychosis shouldn’t get minimized. Living through a stretch where reality completely dissolved leaves marks. Some feel deeply ashamed remembering what they said or did while psychotic.
Others battle persistent anxiety about it happening again, scrutinizing every odd thought or perception for signs psychosis is creeping back. Those reactions are normal human responses to a profoundly jarring experience and deserve therapeutic attention.
Building tougher coping helps guard against future episodes. That means finding healthy pressure valves rather than letting stress pile up. Keeping meaningful social ties going provides support and purpose both.
Sticking to regular sleep schedules matters a lot – sleep disruption frequently comes before and amplifies psychiatric symptoms. Regular exercise helps mental health through several pathways. Dodging alcohol and recreational drugs removes potential triggers for vulnerable people. Working through rough past experiences in therapy can strip their power to spark future crises.
Don’t bail on follow-up psychiatric care too soon. Continuing appointments with a psychiatrist or therapist for several months post-recovery provides ongoing monitoring and backup. Those visits let doctors check for subtle symptom shifts.
They also give patients room to air lingering worries and get reassurance about recovery.
Brief psychotic disorder generally does well when caught fast and treated right. Most people recover completely and never see another episode. While it terrifies everyone when happening, it doesn’t need to define someone’s future or cap what they can achieve in life.
Risk Factors for Brief Psychotic Disorder
Brief psychotic disorder is rare. It usually happens for the first time when people are in their 20s or 30s, and it’s more common in women and people assigned female at birth than in men and people assigned male at birth.
People who have a condition such as antisocial personality disorder or paranoid personality disorder are more likely to get it.
Our Reference based Research
- Diagnosis, Prognosis, and Treatment of Brief Psychotic Episodes: A Review and Research Agenda
- Clinical Outcomes in Brief Psychotic Episodes: A Systematic Review and Meta-Analysis
- Prognosis of Brief Psychotic Episodes: A Meta-Analysis
- Predictors of Diagnostic Stability in Brief Psychotic Disorders
- Reactive Psychoses and Their Overlap with Brief Psychotic Disorder Constructs
- Clinical Characterization of Brief Psychotic Disorder: A Case Series Study
- Psychological and Pharmacological Treatment for Brief Psychotic Disorder with Borderline Personality Disorder
- Brief Psychotic Disorder During the COVID-19 Pandemic: Clinical Descriptions
- Psychosocial Intervention Without Antipsychotic Medication for Brief Psychotic Episodes
- International Incidence and Transition Risk in Brief Psychotic Disorder