



The single most common way an older adult ends up in the emergency room during a heat wave isn’t a fall or a sudden illness. It’s a cascade that builds over two or three days and looks, from the outside, like normal summer behavior right up until it isn’t.
Here’s what it actually looks like. A senior in their late seventies is on a diuretic for blood pressure, like millions of older Americans are. The diuretic does what it’s supposed to do, which is increase fluid loss through urination. In normal weather this is fine.
The body’s thirst signal kicks in when fluid gets low, the person drinks water, the system stays in balance.
Then a heat wave hits. The body loses additional fluid through sweat. The diuretic keeps doing its job on top of that. But the thirst sensation in older adults is notoriously unreliable, and many seniors on blood pressure medications have an even more blunted thirst response than their peers. By day two of the heat wave, the person isn’t drinking nearly enough but doesn’t feel thirsty. By day three, they’re mildly confused but it reads as normal end-of-day tiredness. By the time someone notices something is really wrong, the body temperature has climbed past safe limits and the person is heading to the ER with heat exhaustion or, worse, heatstroke layered on top of significant dehydration.
This cascade is the single most important thing to understand about senior medication safety in summer, because almost every other piece of advice in this space is downstream of preventing it.
Why the Cascade Happens
The cascade has three legs and you need all three to be present for it to develop into an emergency. Take any one of them away and it usually doesn’t.

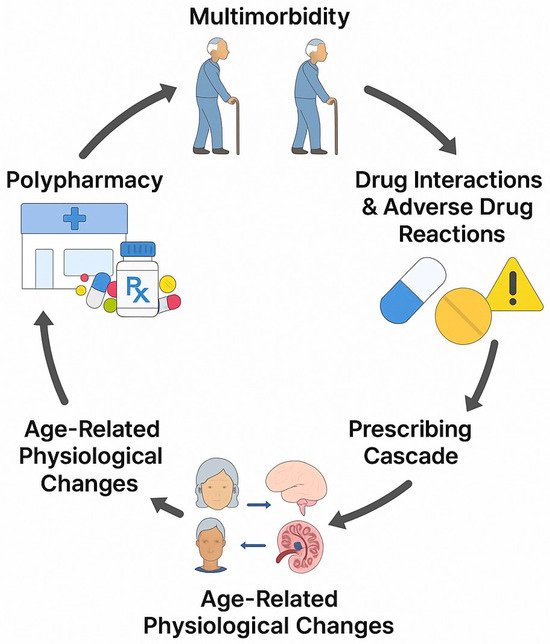
The first leg is a medication that interferes with fluid balance, sweating, or temperature regulation. Diuretics are the most common, but they’re not alone. Anticholinergic drugs (which show up in a lot of antihistamines, bladder medications, and some antidepressants) suppress sweat production directly. Beta-blockers and calcium channel blockers limit how much the heart can ramp up to handle thermal stress. Antipsychotics impair the brain’s own temperature regulation. NSAIDs add kidney stress on top of dehydration. Most older adults on multiple daily medications are taking at least one drug from this list, and many are taking two or three.
The second leg is reduced thirst sensation, which is age-related and not optional. The brain’s thirst signal genuinely gets quieter with age, and the medications mentioned above can make it even quieter. A senior who’s actively dehydrating often doesn’t feel thirsty at all. This is why “make sure they drink water” as advice doesn’t work the way people think it does. You can’t rely on the senior to notice the problem.
The third leg is the heat itself, sustained for long enough that the body’s reserves get depleted. A single hot afternoon usually isn’t enough. Two or three consecutive days of high temperatures, especially with hot nights that don’t allow the body to recover, is where the trouble actually starts.
When all three legs are present, the situation tips. Understanding this is the difference between vague summer worry and actually being able to prevent the emergency.
Drug Categories Worth Reviewing Before Summer

This isn’t about stopping medications. Decisions about medication changes belong with the prescribing physician, full stop. But knowing which medications carry elevated summer risk lets you have a more informed conversation with the pharmacist or doctor.
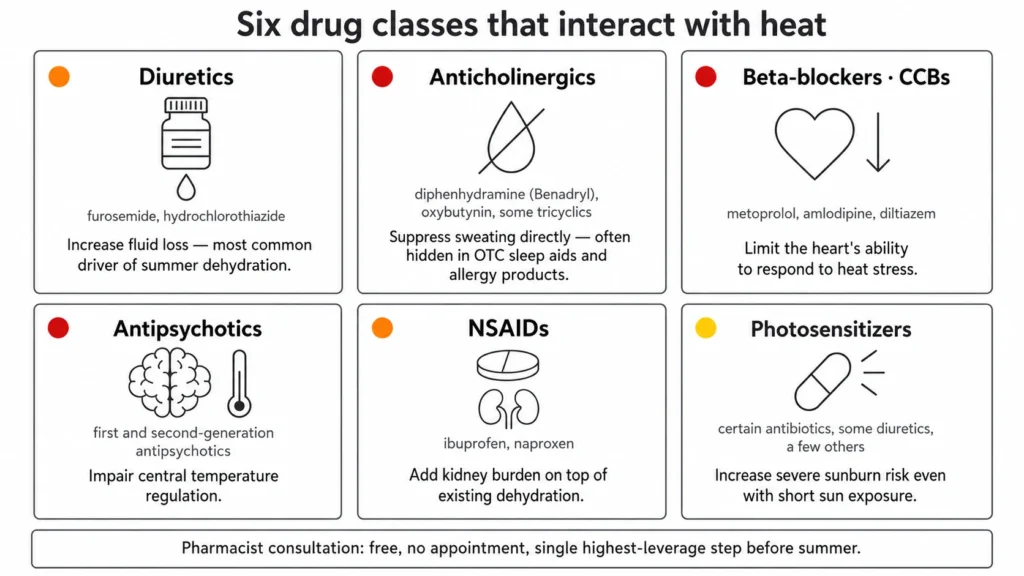
The categories worth being aware of:
- Diuretics (furosemide, hydrochlorothiazide, others). Increase fluid loss. The most common driver of summer dehydration.
- Anticholinergics (diphenhydramine which is Benadryl, oxybutynin, some tricyclic antidepressants). Suppress sweating directly. Often hidden in over-the-counter sleep aids and allergy products.
- Beta-blockers and calcium channel blockers. Limit the heart’s ability to respond to heat stress.
- Antipsychotics. Impair central temperature regulation.
- NSAIDs (ibuprofen, naproxen). Add kidney burden on top of dehydration.
- Photosensitizers (certain antibiotics, some diuretics, a few others). Increase severe sunburn risk even with short sun exposure.
A pharmacist consultation is free, doesn’t require an appointment, and is the single highest-leverage thing a caregiver can do before summer starts. Ask which medications in the senior’s regimen are heat-sensitive, whether any doses should be timed differently during heat waves, and what specific signs of toxicity to watch for given the actual drug combination. Write the answers down. Keep them somewhere visible.
The Storage Side
Medications themselves degrade in heat, which is a separate issue but worth covering in the same conversation. The storage temperature range for most medications is 59 to 77 degrees Fahrenheit, which corresponds to USP standard room temperature. Bathroom medicine cabinets are usually outside this range during summer because of shower humidity and heat. Cars are dramatically outside it. A parked car in summer can hit 130 to 150 degrees Fahrenheit inside within an hour.
The safe spots in most homes are interior bedrooms and dresser drawers away from windows. Refrigerated medications (insulin most commonly) need a plan for power outages, which is a real concern during the heat waves that knock out grid capacity. Ice packs in a cooler buy several hours but not a full day.
Where In-Home Support Changes the Equation
The cascade I described at the top works because nobody is in the room watching for it. Most heat-medication emergencies in older adults happen to seniors who live alone or with a spouse who’s also elderly and similarly unable to notice subtle changes in mental status. Family members checking in by phone can miss confusion because the senior sounds basically fine for the first thirty seconds of a call. The change in baseline that signals trouble is often visible in person but not audible.
This is the part of the picture where professional senior care services materially change the risk profile. A caregiver who visits daily or multiple times a week during summer has actual eyes on the senior, can observe whether they’re drinking water, can check whether the home is appropriately cool, and can recognize the early signs of confusion or dizziness that family members on the phone usually miss. The intervention isn’t medical. It’s observational. Catching the cascade at day one of the heat wave instead of day three is the entire game.
For families with an older adult who’s on multiple daily medications and lives independently, the question of whether to add in-home support during summer months specifically is worth asking. It’s often a smaller commitment than people assume and addresses the exact risk window where most heat-medication emergencies actually happen.
When to Treat It as an Emergency
The symptoms that mean call 911, not the doctor’s office:
- Body temperature above 104°F
- Loss of consciousness or inability to be roused
- Rapid, shallow breathing
- Slurred speech or significant disorientation
Any combination of high body temperature and altered mental status is a medical emergency. Heat exhaustion can progress to heatstroke quickly, and the window for intervention narrows fast once mental status changes.
The article you’re reading is information, not a substitute for medical advice. The pharmacist visit, the doctor’s call, and a clear plan for hot weather are the things that actually prevent these emergencies. Worth doing before the heat hits, not during.