


The hospital figures show up in every Australian sports safety piece and the response from clubs and content sites is identical. Invest in a custom mouthguard. Talk about concussion protocols. Repeat. There is a problem with that response. The custom mouthguard does almost nothing for the brain.
This isn’t a controversial claim inside sports medicine. It’s only controversial inside the gear-sales conversation.
Mouthguards Protect Teeth, Not Brains
A dual-laminate custom mouthguard is excellent at protecting teeth and the mandible from direct impact. That is the function it was designed for and the function the dental literature supports. Where the evidence breaks down is the claim that mouthguards prevent concussion.
A concussion is caused primarily by rapid angular acceleration of the head, the rotational shake that occurs when the skull suddenly changes direction. The dual-laminate sitting against your teeth doesn’t meaningfully change that rotational profile. The Australian Dental Association is careful in how it phrases its position, which is that mouthguards reduce oral and maxillofacial injury. They don’t claim concussion prevention because the evidence doesn’t support it.
The 2014 Study of 6,704 Athletes That Found a 5 Per Cent Crop Per Pound of Neck Strength
In 2014, Christy Collins, Dawn Comstock and Robert Cantu published a study in the Journal of Primary Prevention that ran an anthropometric assessment across 6,704 high school athletes in boy’s and girl’s soccer, basketball and girl’s lacrosse. They used a hand-held tension scale, deliberately chosen as a cheap alternative to a dynamometer so school athletic trainers could actually apply it without specialist equipment.
Their finding, after accounting for sport and sex, was this: every 1-pound increase in neck strength reduced the risk of concussion by 5 per cent.
That’s a dose-response relationship across nearly seven thousand athletes. The intervention costs roughly the same as a pharmacy mouthguard. Practically no amateur club in this country runs the test.
The Mechanism: a Stiffer Head-neck Unit Accelerates Less

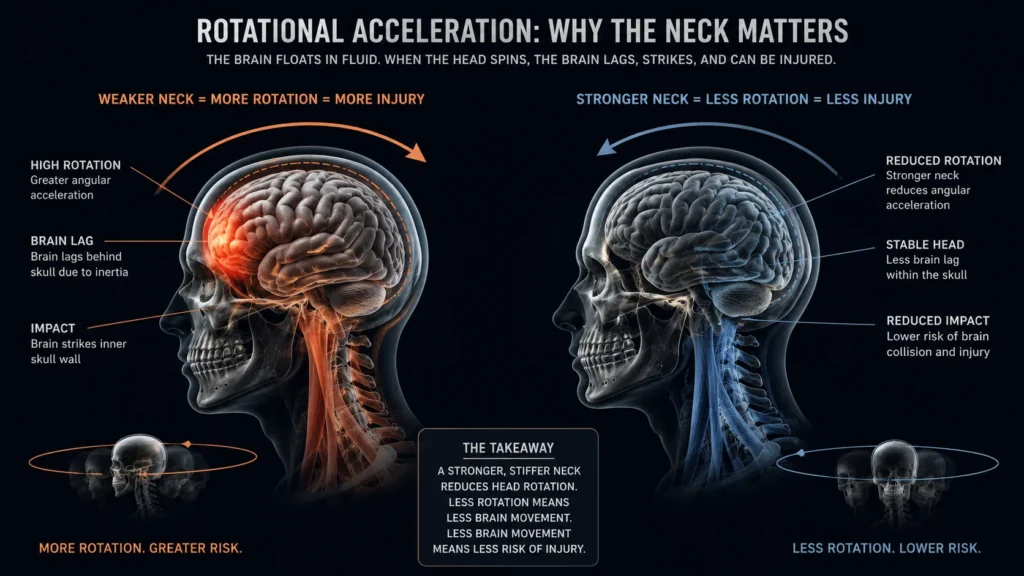
The why is straightforward once you understand what causes a concussion. When a player gets hit, the brain itself doesn’t feel the impact directly. What injures the brain is the sudden rotational and linear acceleration of the skull, which causes the brain tissue to move against the inside of the cranium.
A stronger, stiffer neck increases the effective mass of the head-and-neck system. A heavier object accelerates less from the same force. Translation: your skull moves less, the brain inside it moves less, the injury risk drops.
The instrumented mouthguard work has now confirmed this from another angle. James Tooby and Gregory Tierney’s research group, publishing through BMJ Open Sport and Exercise Medicine across 2023 and 2024, has tracked thousands of head acceleration events using sensors built into mouthguards. High tackles had a 32.7 propensity ratio to cause ball carrier head acceleration events above 30 g compared with medium tackles for men and 41.2 for women. The 2025 rugby league data showed 108 players generating 814 head acceleration events across 468 training sessions, averaging 1.52 events per player per hour.
Tackle height, contact geometry and how well the head-neck unit resists the resulting acceleration. Those are the variables. Mouthguards are excellent for measuring the problem now. They were never the solution to it.
What the AIHW 2023-24 Figures Actually Show
The current AIHW data is worth reading carefully. In Australian rules football, head and neck accounted for 23 per cent of hospitalisations, or just over 1,200 cases. Intracranial injuries made up 7.5 per cent of admissions, about 405 cases and roughly 96 per cent of those were concussions.
The female-versus-male picture is more pointed. The rugby codes had concussion hospitalisation rates 1.6 times higher for females than males. Factors influencing this include physiological differences such as reduced neck strength, recent rapid increase in female contact-sport participation and greater likelihood of reporting and seeking health services.
A signal pointing directly at neck strength as a modifiable risk factor, in the population most affected, in the data the safety conversation already quotes. The conversation hasn’t caught up to what the data is actually saying.
What a Tension Scale and a Printed Protocol Costs an Amateur Club


A hand-held tension scale and a printed protocol for isometric flexion, extension and lateral neck testing costs less than fitting a single player with a dual-laminate mouthguard. Twice-a-season testing, with a simple cervical strengthening warm-up integrated into training, is the most evidence-supported concussion intervention currently available to a community-level club.
The mouthguard stays in. It protects teeth and jaws, which the AIHW data makes clear are at real risk and expensive to fix. Just stop selling it as a concussion product. The cervical muscles are doing the work the mouthguard was being credited for.